
Sharing things, whether food, a toy, a sympathetic ear is a way of showing caring. Indeed, the Salvation Army has trademarked the phrase “Sharing is Caring” to cover their activities as a religious organisation supplying food to needy families, gifts for patients in hospitals and care homes and toys for underprivileged children. This is sharing of good things, by those who have, with those who lack.
This concept of sharing to help others is a worthy aim, that trips easily off the tongue. In practice humans find sharing difficult and it is not an innate characteristic. The pleasure of giving to others and the ability to share with others is something we learn as we grow up. Ask any parent resolving an argument between siblings over a toy. It has even been known for parents to buy two toys to prevent quarrelling.
At the moment, this phrase is probably not foremost in our minds. More likely we are thinking more about sharing the difficulties and stresses imposed by living through the Covid pandemic and our caring has been expressed more in appreciation of those working on the front line, particularly those in the health service. We also acknowledge those in the course of their work, whether as couriers/postmen, supermarket workers, teachers etc, who are exposed to greater risk than the general public because they interact with a large number of people each day. However, this caring does not require a sacrifice on our part.
We, the public, have been told by our governments, to care for others by following the guidelines to save lives. We are also told regularly that we are “all in it together for the long term” and that the virus does not respect national boundaries. “In it together” holds as far as the fact that the pandemic affects us all, but it implies that we are all pulling together in the same direction across different sections of society, both within the four countries of the UK and across the world. This is of course untrue, as governments and political parties debate the right course of action in a rapidly evolving situation. Whilst the majority in the UK have been remarkably law abiding in sticking to the restrictions, there is a groundswell of support for a review of how our government has handled the various issues, how life in the UK has been affected and whether the Government has fulfilled its responsibility to keep us safe. A Peoples Covid enquiry, chaired by Michael Mansfield QC, began on March 3rd and eight on-line sessions on the the following topics are planned:
- How well prepared was the NHS?
- How did the Government respond?
- Is ‘Zero Covid’ possible?
- Impact on the population 1 (families, social care, disability)
- Impact on frontline staff and key workers
- Inequalities and discrimination
- Privatisation of the Public’s Health
- Impact on the population 2 – (schools, young people, women and mental health)
It will be interesting and important that this review answers these questions and provide lessons for the future that are learnt. We already know that preparation for the pandemic was inadequate with money provided for future potential pandemic planning diverted elsewhere and that governments have a tendency to rewrite history and to mitigate or deny self-blame. The overall success of the current UK vaccination programme has pushed the failures of PPE supply and mistakes over protection in care homes – to cite just two examples – to the background. Any subsequent government review will be scrutinised very carefully because the cost to communities and to individuals has been so high and will continue for some time. At the time of writing there have over 4 million Covid cases and over 124,000 deaths in the UK . There has also been immense financial, mental health and other costs to individuals. The sheer scale and length of this crisis has led to extensive documentation by many different groups and individuals. Hopefully, this will ensure that history is not rewritten for the party in power.
It is ironic that while governments publicise that “the virus knows no boundaries”, the fight against Covid-19 has been very much compartmentalised within national boundaries. This is despite world organisations such as WHO arguing against this approach. On March 13th 2020, two days after WHO had declared that Covid -19 was a global pandemic, the UN Secretary General issued a statement stressing the need for global co-operation with the basic message that “we are in this together – and we will get through this, together.“ Within this statement he stated that “no country could do it alone and that governments must cooperate to revitalise economies and provide support for the people and communities most affected by the disease. A pandemic drives home the essential interconnectedness of our human family. Preventing the further spread of Covid-19 is a shared responsibility for us all. “The cost for this has been estimated at $22.9 billion.
It is a year since that statement and only within the last few weeks has there been much evidence of these words being heeded. Individual countries have concentrated on measures to control the spread of infection, to reduce mortality and to prevent hospitals from being overwhelmed by severe cases. Now following the amazingly successful research, development and administration of vaccines the situation has started to change. In the UK three vaccines are licensed for use (Oxford/AstraZeneca. Pfizer/BioNTech and Moderna) with options for four more already taken up (Novavax, Valneva, GSK/Sanofi Pasteur, Janssen (Johnson) -the last is already approved in the US. Throughout the world there are 23 approved vaccines including Sputnik V and Sinovac (CoronaVac) and a further 56 in development.
There is plenty of good news about the vaccines in terms of efficacy. Studies both in England and Scotland show that a single shot of either the Oxford-AstraZeneca or the Pfizer-BioNTech vaccine jab reduces the chance of needing hospital treatment by more than 80% . However the roll out of vaccines across different countries varies widely.
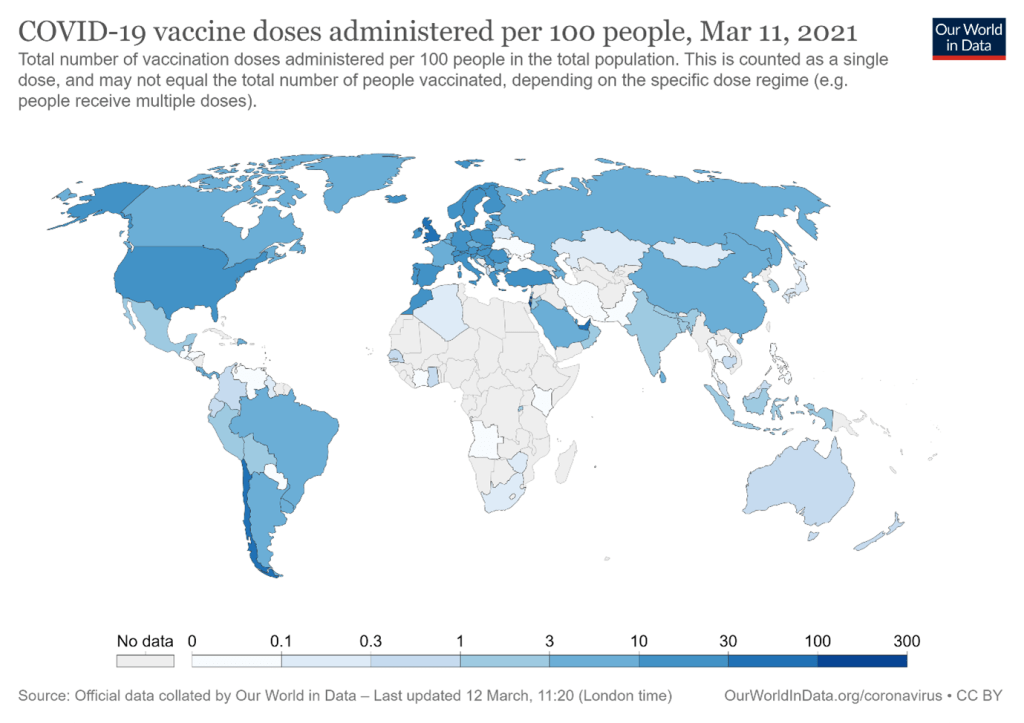
In Israel over 93% of the population have been vaccinated . In the UK the figure is around 31% and the US has improved vaccination coverage significantly in recent weeks to reach 22% *. By contrast in less developed countries the figure is very much lower and even India with a good manufacturing capacity itself has only achieved 1.6%. The figures provided by Our World in Data do show daily improvements but as can be seen from the map there are very marked inequalities. The International Federation of Red Cross Organisations (IFRC) has warned of “ a glaring gap in COVID-19 vaccine roll-out” and has raised only 3% of the US$111 million needed to meet its target of vaccinating 500 million people across the world. Overall, the availability of vaccines is extremely patchy and there is a long way to go before every country can feel their citizens are protected against the disease.
The inequalities caused by the limited availability of vaccines, the inefficient distribution and administration of them in various countries has led to a lot of rancour and disunity. At the end of January, WHO asked the UK to share its vaccine supply with poor countries, once the vulnerable population had been vaccinated (as has now been achieved). Within the EU there have been complaints about the so-called unified vaccine approach and contradictory statements and decisions made. There have been disagreements within the EU and between the EU and the UK. All this has shown how far we are from embracing the sharing and caring concept in practice.
The disunity within the EU has been particularly marked despite the setting up of a single body to purchase vaccines on behalf of the 27 countries in June 2020. The EU roll out has been poor compared with the UK vaccine programme: France, Italy and Spain for example have each only delivered one quarter of the number of vaccinations as the UK. A number of factors have contributed to this state of affairs: low precommitment to purchase of vaccines, lack of investment in vaccine research, slow regulatory approval of vaccines, and spreading adverse publicity on the Oxford/AstraZeneca vaccine.
At the end of January France’s President, Emmanuel Macron, claimed that the Oxford/AstraZeneca vaccine was “almost ineffective” for over-65s and this was echoed by Angela Merkel. The Germans made a draft recommendation that the Oxford/AstraZeneca coronavirus vaccine should not be used in over-65s.This resulted in a lack of confidence in the vaccine amongst French and German people, with 40% seeing the vaccine as unsafe and a very low attendance at vaccination clinics. Of 1.5 million does available only 150,000 had been used. It was not until very recently that both French and German authorities permitted it’s use in the over 65s and France has stated it would “rehabilitate” the vaccine. France and the EU have failed to secure a deal this year for the French vaccine Valneva, which has a manufacturing plant in Scotland. By contrast the UK has secured 100 million doses. In addition to all this there have been two separate vaccine export rows. In the second, the President of the European Council wrongly claimed the UK had paced an “outright ban” on exports of vaccines produced in the UK.

These rows on vaccine administration have resulted both in poor roll-out figures in the EU and lack of confidence in the system and in the European Medicines Agency (EMA) to the extent that individual countries within the EU are rebelling against the joint scheme and seeking individual vaccine deals. For example, Denmark and several other countries are seeking vaccines from Israel, which has an excess of Moderna vaccine. Eastern European countries, such as Hungary, Slovakia and the Czech Republic, are in the grip of a third wave of the coronavirus pandemic and unsurprisingly seeking vaccines from Russia and China not yet approved by the EMA, in addition to 100,000 doses of the Pfizer/BioNtech under the EU recovery scheme. For example, Hungary has approved use of the Russian Sputnik V vaccine.
The whole situation is redolent of a splintered process. Those countries with excess vaccine can use “vaccine diplomacy” to improve relations and influence other countries. In addition, there is the potential for the development of black markets and anarchy in vaccine distribution. This is a far cry from the calls from WHO, UN, and the IFRC , who have each advocated a unified and fair joint approach. The Italian economic minister, Daniele Franco, said in late February 2021: “We will not get back to our normal lives until the virus is eradicated in all countries,” adding that fellow ministers had agreed on the necessity of a “bold and global response aimed at curbing the virus diffusion everywhere.”
A unified approach for equable vaccine distribution does exist – the Covax scheme. This scheme was set up by WHO, the Gavi vaccines alliance (founded in 2000) and the Coalition for Epidemic Preparedness Innovations (CEPI) to help poorer countries. Based on the mantra “With a fast-moving pandemic, no one is safe, unless everyone is safe “ the COVAX scheme , designed not only to provide equitable sharing of vaccines among the world’s population but also to accelerate the development and manufacture of COVID-19 vaccines. Covax is aiming to deliver about 2 billion doses of Covid-19 vaccines globally by the end of the year to 92 lower-income economies. The scheme was launched in June 2020 and after an initial slow start it has been gathering speed as richer nations feel more secure in their own vaccine supplies.
Ghana was the first country to receive Covid vaccines on February 24th 2021 with 600,000 doses of the Oxford/AstraZeneca vaccine arriving. Within two weeks 162, 000 vaccinations had been administered, reaching 1% coverage. At the start of February the vaccination coverage in African, Asian and South American countries was almost non-existent but by March 11th has reached around 3% in Asia but still only 0.5% overall in Africa. . In total 28.5 million doses of vaccines have been delivered to 37 countries, including 11 African countries, Brazil, Afghanistan, Indonesia, Cambodia and Tajikistan. The scheme has about $7.5 billion (£5.4 billion) pledged and received a major boost after the February G7 summit with the US, Germany, the UK, France and the EU pledging significant sums.

Photo credit UNICEF/ Francis Kokoroko
However, there is still a long way to go both in providing a unified approach and in delivering vaccines. . Max Lawson, Oxfam Head of Inequality Policy, said: “While some of those attending the G7 have made welcome steps to increase the supply of vaccines to poor countries, these remain insufficient when compared to the scale of the Covid-19 threat”. The dangers of vaccine nationalism and “vaccine diplomacy” need to be addressed. Even if the full roll out of 2 billion Covax doses is achieved this year, more is needed to vaccinate the world population of 7.8 billion for the first time around.
So, as we envisage the prospects of being able to co-operate on Covid vaccination across the world and support a scheme goes against the natural grain of looking after our own interests first, it is relevant to consider two points. First, can we cite any examples where caring for the disadvantaged benefits the population as a whole and, secondly, are we likely to need such global co-operation again in the future?

In nature trees in forests have extensive interconnections provided by a fungal network that enables exchange of nutrients, sending of chemical messages and providing defences against pathogens. As Peter Wohllleben explains in his book “The hidden life of trees“, it is beneficial for the community as a whole to succour weaker neighbours. Isolated trees are much more open to attack by fungal and insect predators.
It is foolish to expect that once the Covid pandemic is over we can all relax. Scientists predict that in the future pandemics will occur with increasing frequency as human behaviour increases the likelihood of viruses adapting to new hosts. In his programme “Jump”, Chris van Tulleken explores how and why this happens. In addition, we know that existing worldwide problems such as hunger and poverty have been exacerbated by the current crisis. Add in water shortages, climate change and depletion of scarce natural resources and it is likely we will face crises of equal magnitude in the future.
Will we react concertedly in a caring/sharing manner and be prepared to make some sacrifices or will we forget the lessons we have learned once the crisis is over?
Written 3rd-14th March 2021
